





2023-02-20 00:00:00
ULNAR COLLATERAL LIGAMENT RUPTURES
Ligaments are structures of soft tissues that connect bones to each other.The ulnar ligament is ...


A greenstick fracture refers to bending or at most cracking a bone, instead of simply breaking into separate pieces, as it happens in a usual fracture. Greenstick fracture frequently occurs in younger children, because their bones are softer and much more flexible compared to adult bones.
In some cases, this type of fracture can be quite difficult to diagnose, as there are no symptoms specific to a fracture - pain and tumefaction (local swelling). Since the child will often be able to use the affected upper limb freely, he/she will not realize that there is a problem. Only more severe forms of greenstick fractures can cause obvious deformation, significant pain and swelling.
Light greenstick fractures are often confused or even considered to be sprained, but the difference must be made between a greenstick fracture and a sprain.
Most greenstick fractures are found in babies and young children, up to the age of 10. Even if the bone is not completely fractured, immobilization with the help of a splint or plastered apparatus is necessary both to accelerate healing and to prevent complete breakage, in case the child falls again on the injured forearm.
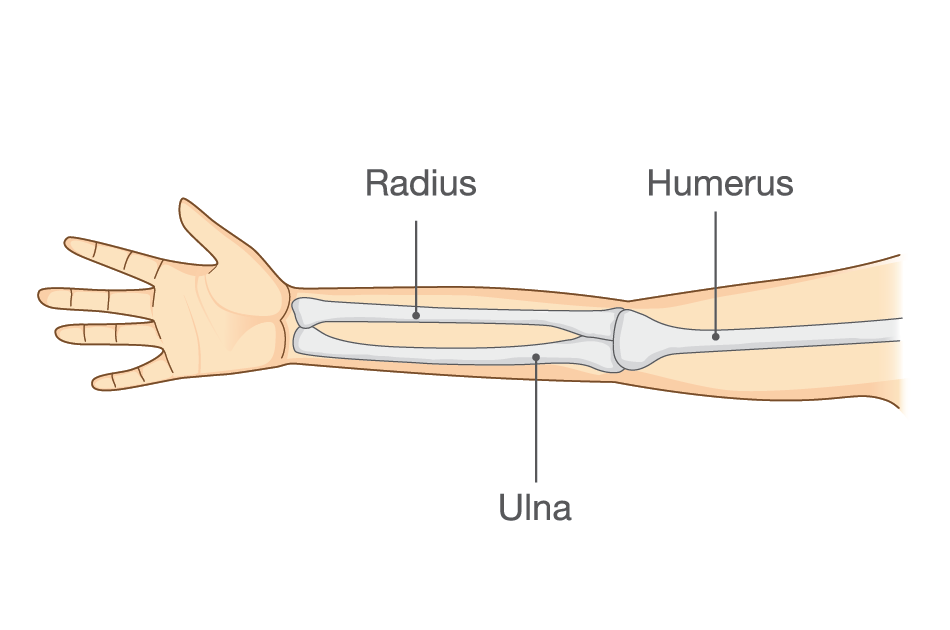
The forearm consists of 2 bones, radius and ulna.
Fractures of the forearm bones occur either near the wrist known as the distal fracture or in the middle part of the forearm or near the elbow in the upper portion of the bone, known as the proximal fracture.
Distal radial fractures are generally the most common types of bone fractures, the distal end of the radius bone being located near the wrist.

If a child falls on the stretched upper limb, he/she could end up breaking one or both of his forearm bones. Greenstick fractures encountered in children are the result of falling off bicycles and trampolines or colliding during contact sports.
Lighter fractures only need a plastered splint to allow the bones to heal.
In the case of fractures that are more severe and inclined, the closed reduction is attempted (repositioning the bones in their normal position), provided that the bones have not pierced the skin. Stable fractures (without displacement of the bone ends) require up to 3-4 weeks of immobilization in the gypsum apparatus. The more serious the injuries, the longer the period of immobilization increases, up to 6-8 weeks.
It is an option for realigning the bones in their normal position if they have pierced the skin, the fracture is not stable, the bone segments are displaced, the bones have begun to heal improperly, or the bones cannot be aligned only by closed reduction.
Both after immobilization and after surgery a specific exercise program helps regain the mobility of the affected upper limb.
➢ Regular exercise and a good diet help build strong bones. Calcium and vitamin D3 have an important role in building strong bones
➢ The equipment appropriate to each sport helps prevent injuries
➢ Falls on the extended arm will be avoided as much as possible

I always follow professional workflow and provide you the best service with reliable costs.



Ligaments are structures of soft tissues that connect bones to each other.The ulnar ligament is ...
The meniscus rupture is one of the most common knee injuries . Any action or activity that involves twisting or rotating ...
The rotator cuff is a tendinous blade that covers the anterior, upper and posterior side of the shoulder ...


